


Mohammad Ali Leghari1Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS, MSPH
Farzeen Tanwir2Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Post-Doc, PhD, MPhil, C.Orth, BDS
Humera Ali3Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â Â BDS
OBJECTIVE: To evaluate the association of oral health knowledge of parents in relation to dental caries of their children.
METHODOLOGY: This cross sectional study was undertaken in Malir Town, Karachi. Oral examination of 399 school going children enrolled in local private schools was carried out to assess their dental caries status. A Selfadministered questionnaire was used to gauge oral health knowledge of parents.
RESULTS: Study sample comprised of 49% boys and 51% girls. The prevalence of dental caries was 70 % with a mean DMFT score of 1.4. was significantly higher among girls compared to boys. The dental caries increased as the age increased from 12 year age to 15 year. Parents were aware that regular visits to dentist can prevent dental caries but there were large numbers of parents who visited dentist when there was the pain in teeth.
CONCLUSION: The current study found that female students had relatively higher odds of dental caries than compare to males. Parent’s knowledge of oral hygiene had effect on their children oral health. Oral health programmes should be performed in future for the oral health care awareness for both children and their parents.
KEY WORDS:Â Dental caries, socio economic status, parents dental knowledge. DMFT
HOW TO CITE: Leghari MA, Tanwir F, Ali H. Association of dental caries and parents knowledge of oral health, A cross-sectional survey of Private Schools. J PAk Dent Assoc. 2014;23(1):19-24.
INTRODUCTION
The distribution of dental caries has changed dramatically in last few decades shifting its base from developed countries to developing countries. Dental diseases are the most expensive to treat and rank fourth in developed countries1. Dental caries that is left untreated can affect children’s quality of life, as untreated caries cause discomfort, pain, dental sepsis and as a result loss of school days2.
The prevalence of dental caries in developing countries has been attributed to less number of preventive programs in the community and in schools, lack of water fluoridation; in-efficient oral health care arrangements and consumption of refine carbohydrates. The higher number of dental caries in developing countries is mainly attributed to urbanization and socioeconomic factors3.
Good oral hygiene is imperative factor prevention of dental caries. There is little known of the oral health knowledge of the school going children in developing countries3. Recently, it has been reported that the dental health status of the children is affected by dietary habits and the social class of their family and the maternal education4, 5, 6,7.AL-Hosani reported low caries prevalence in children of parents having high education level and better socio-economic status8.
Federal surveys report of US Surgeon General’s workshop, “Children and Oral Health,†found that there were disparities in the oral health of the children and the access to dental clinic for treatment for dental cavities and there were 60 % more untreated dental diseases compared to high income group9.Factors like parents low education, unemployment and low income are also associated with the poor health and chronic diseases10.
The study of Tickle et al.11 conducted on children who were registered to general dental clinic in north of London, stated that children belonging to poor environment experience higher dental caries, and are less likely visit to dental clinics Moreover, children who visit dental clinics more often have lower incidence of dental disease although they score higher for treatment done.
There is scarcity of data on oral health knowledge amongst parents and its association with dental health status of their children. The last nationwide survey was done in 2004 in different cities of Pakistan, since than no major project has been undertaken12.
The main objective of this study was to find out the prevalence of dental caries in school going children aged 12 -15 in relation with the oral health knowledge of their parents. The results of this study could be used for evaluating health services and planning oral health related programs in Malir district.
METHODOLOGY
An analytical Cross sectional study for the assessment of dental caries was conducted in school going children aged 12-15 years in Malir town, Karachi. A sample size of 380 was calculated based on previous prevalence study done by A.A khan in Lahore 13 and following formula  was used for the calculation of the study sample size14. A standard Error of 5%, a confidence interval level of 95% and an Expected prevalence of 55% was used. There are seven Union councils in Malir town, two schools from each union council were selected by convenience sampling, and from each school 28 children were selected by simple random sampling Sample size was increased from 380 to 392 due to the extra examination of the participants to prevent the dropout during the study. The head masters of selected schools were contacted and their consent was obtained for participation in the study.
Malir town is considered a low socio-economical area of Karachi, although there is no data available that specify standardized socioeconomic status of the different towns of Karachi. For clinical dental examination, specifications recommended by “World Health Organization (Oral Health Survey Basic Methods, Geneva 1997) for Oral health surveysâ€15 were used as at this age, all permanent teeth have had erupted.
The study tools comprised of self structured, close ended questions adopted from articles and research studies of similar design, and was modified accordingly to assess parental oral health knowledge. These questionnaires were translated into Urdu language for the ease of understanding of the respondents. Urdu is the national and official language of Pakistan 16 and majority of the population of Pakistan understands it. The questionnaires for parents were handed over to the children who carried it to their home for their parents. Those questionnaires were filled by parents and children brought them back to the school and were collected from the school, the next day.
Basic oral examination instruments namely mouth mirror, dental explorers CPI probes and a dental lamp were sterilized for the detection of dental caries following strict cross infection control protocol. Oral examination was done by single operator to detect the presence of dental caries, missing (extracted or congenital) and filled teeth. All 28 permanent teeth were examined excluding the 3rd molars.
Description of frequencies and proportions of discrete variables and mean (SD) for continuous variables were presented for dental caries of children. T-test was applied for differences of mean for categorical variable. Univariate and multivariable logistic regression analysis was applied to check the association of parent’s knowledge with dental caries. The DMFT variable and completed questionnaires were then entered in STATA version 11 for statistical analysis.
RESULTS
The response rate of parents was 38% (n=150) therefore the information on parent’s oral health knowledge is limited to 150 participants. Of the 150 students examined, 73 (49%) were boys and 77(51) girls. The frequency of age distribution was 15(10%) 12 year age, 36(24%) 13 year age, 39(26%) 14 year age, 60(40%) 15 year age.
The overall mean DMFT score was 1.4 (.10), scores of dt, mt and ft components were 1.17(.09), .05(.02) and .15(.03) respectfully. The mean DMFT in boys was 1.06 and in girls it was 1.45. The DMFT value by age stratification showed that DMFT value was 1.33 in 12year and 13-years old and 1.41 and 1.45 in 14- and 15years old children respectively. The study showed that as the age of the children increased from 12 to 15 years the DMFT value was also increased (see table 1).
Student’s distribution according to father education was categories into less than 10 year education consists of (33)22% students, 11-12 year education (74)49% and education greater than 12 year was (43) 29%. On the other hand student’s distribution by mother’s education
Table 1:Â Mean DMFT (SD), D-T, M-T, and F-T and frequencies of DMFT by age and sex.

Notes: DMFT= decayed, missing, and filled teeth; DT = decayed teeth; MT = missing teeth by caries; FT = filled, *p-value <0.05 was (59) 39 %, (74) 49% and (17) 12% according to lower, middle and higher education categories.
Family income was categories according to income less than 15000 Rs and income greater than 15000 Rs and there were 47(31%) and (103) 69% students respectfully.
The independent variables included student’s gender, student’s age, parent’s level of education, income and knowledge of parents and dependent variable was prevalence of dental caries. The variables were categories into socioeconomic status, child variables and oral hygiene knowledge. It was observed that odds of dental caries was less in female students as compare to male although the results were not significant p value was greater than .05. The odds of dental caries were also increased with increasing age of the child, parent’s education level and household income, however the results were insignificant.
In response to the question asked from the parents regarding the knowledge of plaque, 80(53.3%) said that
plaque was the remaining of the food particles that sticks to the teeth, 49(32.7%) considered plaque and stains as synonymous, while 21(14%) did not know what plaque was.
As for the effect of plaque on teeth, 62(41%) parents considered plaque as a cause of dental caries,40(26.7%) considered it a cause of bleeding gums, 33(22%) responded that plaque discolours the teeth whereas 15(10%) did not have any knowledge about the oral effects of plaque. Regarding factors leading to dental caries, 38(2%) stated bacteria, 37(24%) chose sweets, 22(14.67%) stated sugar, while 23(15.3%) highlighted frequent snacking as a causative factor whereas 23 (15.3%) did not have any knowledge concerning factors leading to dental caries presented in table 2.
It has also been observed that 139(92.6%) parents used tooth-brush and toothpaste devices for the cleaning of their children’s teeth whereas 11(7.3%) used Miswak tool for the cleaning of their teeth. While, 97(65%) used fluoridated toothpaste and the other remaining 53(35%)
Table 2:Â Mean (SD), proportion of children with dental caries in relation to oral knowledge of parents.

did not use a fluoride toothpaste. T-test for variable regarding knowledge of fluoride and mean DMFT in children presented in table 3.
When asked from the parents if brushing teeth prevents caries, 114(76 %) answered ‘Yes’ as a response. The odds of dental caries was 2.29 times more in children in those parents who said that fluoride had no effect on protection from dental.
The odds of dental caries were higher in children not using fluoridated toothpastes. The odds of dental caries in children were higher (OR= 2.3, p value= .034) if their parents answered that fluoride doesn’t prevent dental caries.
Multivariable logistic regression analysis. After adjusting for other variable the odds ratio of dental caries was statistically significant for father education and children’s gender. Boys were significantly more protective
Table 3:Â Parental knowledge of fluoride with mean DMFT of their children
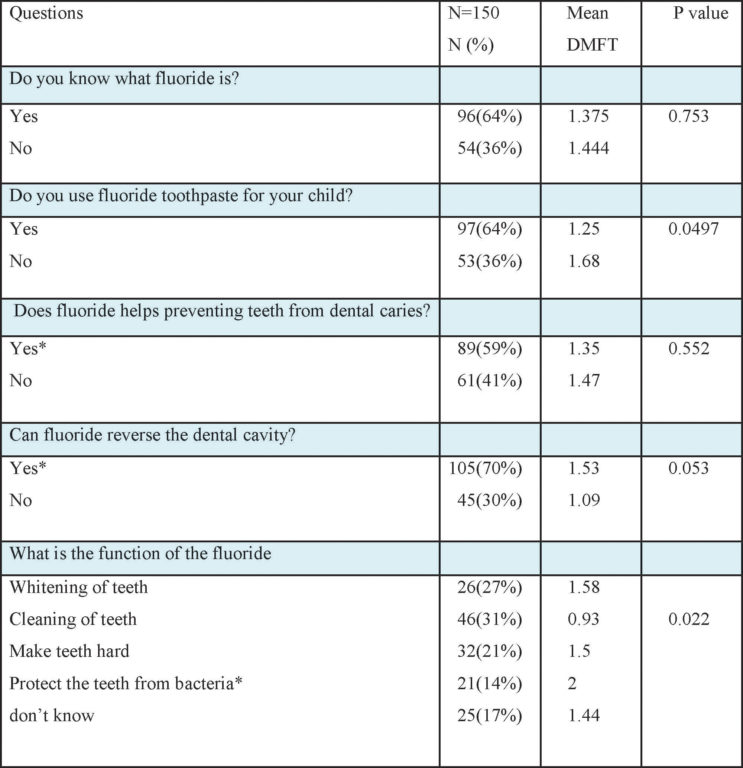
Table 4:Â Univariate and multivariable logistic regression model to calculate OR for children’s characteristics effect on dental caries (N=150).
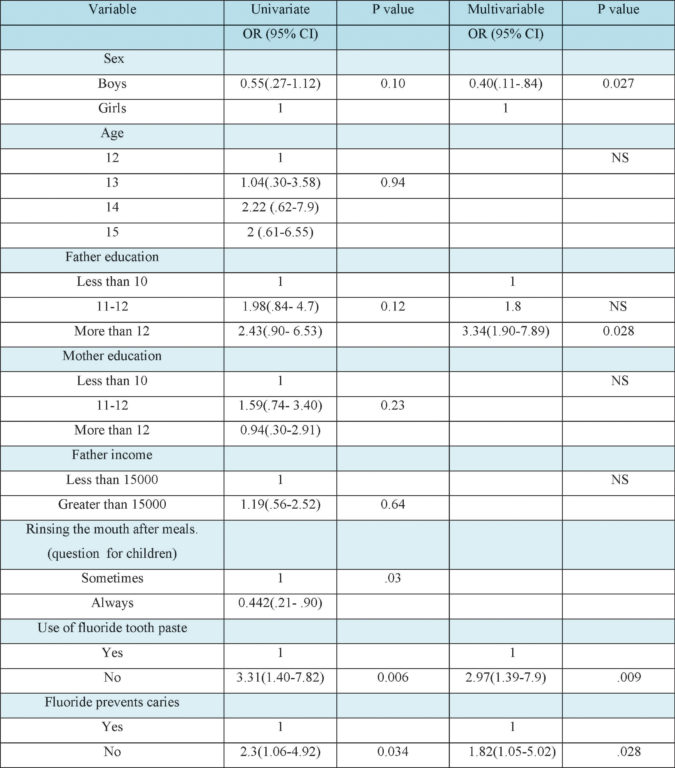
for been free from dental caries. The OR of dental caries increased while father’s education increased. The OR of dental caries was 3.34 for children with father’s high education compared to children with fathers who have low education (table 4).Those parents who didn’t use fluoride tooth paste the odds of dental caries was 3 times higher than those who used fluoride toothpaste (P=0.009, Table 3). The knowledge of parents about fluoride was significantly associated with occurrence of dental caries and those who didn’t know about this fact had 1.82 times higher odds to get dental caries compared to those who knew (P=0.028, Table 4).
DISCUSSION
The mean DMFT index score was 1.4 and was smaller than the previous national health survey of Pakistan (NHSP 2004) which was 1.6 12 .The prevalence of dental caries was 70% which was almost similar to the study that was carry out in Kenya17 but was higher from oral health survey that was done in 2004 where it was 50%12. Eating habits between meals and after meals was the same for boys and girls and the results showed the similarity to the study that was done in school going children in U.A.E 8.
High income parents who do not have proper oral hygiene knowledge have higher odds of occurrence of dental diseases in their children. The combination of high income and poor parental education is a new risk factor which needs further investigation. Same phenomenon was also seen in children in Abu Dhabi where the students had the high dental caries status in high income families8.
There were disparities of knowledge of oral health in girls and boys and the results were similar in study done in Japan18.The study reveals that girls had more knowledge and were more oral health conscious as compared to boys but the mean DMFT score was greater than boys. This is more likely due to the socioeconomic status, and girls were from the families where there were no gender differences with regard to priorities for attainment of education between girls and boys. National health survey in Hungary also found out the gender difference in dental caries experience and in the increase of prevalence of caries and as age increases which is the same as our study19.
The DMFT index score increased as the father and mother education increased from lower to intermediate but it decreased in the parents with higher education. The mothers of the children with higher education had lower DMFT index score as compare to the other intermediate and lower education groups. Previous studies also reported similar DMFT in different education groups 20. But there were contrasting results regarding association the DMFT score with high level of income. Children belonging to higher household income had high DMFT score, and On the other hand, high income also related to the higher decayed, missed teeth surprisingly there were also higher numbers of fillings present on their children teeth with high level of income. It reflects that consumption of sugar and cariogenic food was increasing as the income increases and causing more teeth decay to occur as well as perception of visiting to dental clinic increases for the restorative treatment. There was no significant relationship seen in parent’s socio demographic characteristics with the mean DMFT of their children. There was less numbers of participants in the study and there was less power to reject the null hypothesis.
It has been seen that children belonging to families with high socio economic status had a higher DMFT, score and had more fillings presents on their teeth as compared to their counter parts from low socio economic status group. The poor status was not the factors for the occurrence of dental diseases but it was the high income that led the disease to occur and drove them towards dental clinic for dental filling treatment. These results were dissimilar and contradictory from the study done in USA21. In response to the question about the effect of fluoride on teeth, 46% of the parents said that it cleans and helps in whitening of teeth. Similar wrong perceptions were reported in another study (Kingdom of Saudi Arabia)22.
Even though the sample size was very low, the current study has a great potential to be used as a pilot study23 in future research projects in Pakistan. The descriptive results can have important policy implications and that is the major contribution of the current study in future plans of oral health programs among school children in Karachi. Parents were aware that regular visits to dentist can prevent dental caries but there were large numbers of parents who visited dentist when there was the pain on teeth. There were some parents who said that they prefer to visit physicians for dental consultation.
In Pakistan there was not very much work done on national level for the evaluation of oral diseases in school going children, the last survey done in 2004 in different cities of Pakistan. There was not any study carry out on this topic and publish in local or international journals. This is the first study that focuses on both children and parents knowledge variables with relation to the dental caries in Karachi, Pakistan. This study can be baseline or reference study for the conduct of further studies in future in Pakistan.
For parents there were some variable which had significant effect of oral hygiene to their children dental caries. The role of mother particularly those who are educated with advanced education should not be neglected and have important role in taking care of oral hygiene of their children.
CONCLUSION
The prevalence of DMFT was higher in girls than compare to boys and the results were statistically significant. The DMFT status of the study population increases as the age of the students increases. Parents had moderate amount of knowledge regarding fluoride and also had some effect on their children’s dental caries status. Rinsing the mouth after taking the food and the use of fluoride containing toothpaste was protective against the cariogenic activity.
REFERENCES
- http://www.who.int/bulletin/volumes/83/9/editorial 30905html/en/index.html(accessed on 25th January 2012).
- Williams N. The relationship between sociodemographic characteristics and dental health knowledge and attitudes of parents with young children. Brit Dent J. 2002; 193:651-564.
- Varenne B, Petersen P, Ouattara S. Oral health behaviour of children and adults in urban and rural areas of Burkina Faso, Africa. Int Dent J. 2006; 56:61-70
- AS Doddamani, Prashanth VK, Abbayya K, Yunus GY. Oral Hygiene Status Among School Going Children Belonging to Different Socio-economic Status of Belgaum City Aged 12 To 15 Years. JIDA, Vol. 4, No. 12, December 2010
- Sogi GM, Bhaskar DJ. Dental caries and Oral Hygiene Status of school children in Davangere related to their Socio – Economic levels: An Epidemiological study. J Indian Soc Pedo Prev Dent December 2002;20: 152-157
- Oliveira LB, Sheiham A, Bönecker M. Exploring the association of dental caries with social factors and nutritional status in Brazilian preschool children. Eur J Oral Sci 2008; 116: 37-43
- Marrs JA, Trumbley S, Malik G. Early Childhood Caries: Determining the Risk Factors and Assessing the Prevention Strategies for Nursing Intervention.Pediatr Nurs.Pediatr Nurs. 2011 Jan-Feb; 37:9-15; quiz 16.
- Al-Hosani E, Rugg-Gunn A. Combination of low parental educational attainment and high parental income related to highcaries experience in pre-schoolchildren in Abu Dhabi. Community Dent Oral Epidemiol 1998; 26:31-36
- Karjalainen S, Söderling E, Sewón L, Lapinleimu H, Simell O. A prospective study on sucrose consumption, visible plaque and caries in children from 3 to 6 years of age. Community Dent Oral Epidemiol 2001; 29:136-142.
- Figueiredo M, de Amorim R, Leal S, Mulder J,Frencken J. Prevalence and severity of clinical consequences of untreated dentine carious lesions in children from a deprived area of Brazil. Caries Res. 2011; 45:435-442.
- Tickle M, Williams M, Jenner T, Blink horn A. The effects of socioeconomic status and dental attendance on dental caries’ experience, and treatment patterns in 5-year-old children. Brit Dent J. 1999; 186:135-137.
- World Health Organisation-WHO. Oral Health in Pakistan-Situation analysis. Ministry of Pakistan: 2004; WHO.
- Khan AA. Prevalence of dental caries in schoolchildren of Lahore, Pakistan. Community Dent Oral Epidemiol. 1992; 20:155
- Daniel WW. Biostatistics: A Foundation for Analysisin the Health Sciences. New York: John Wiley & Sons; 1999.
- Methods World Health Organization. Oral HealthSurveys. Basic Methods, 4th edn.Geneva, Switzerland: WHO, 1997.
- United state department of state: http://www.state.gov/r/pa/ei/bgn/3453.htm (accessed on 25th January 2011)
- Masiga MA1, M’Imunya JM.Prevalence of dentalcaries and its impact on quality of life (QoL) among HIV-infected children in Kenya. J Clin Pediatr Dent. 2013; 38:83-87.
- Kawamura M, Takase N, Sasahara H, Okada M.Teenagers’ oral health attitudes and behavior in Japan: comparison by sex and age group. J oral sci. 2008; 50:167-174.
- Szöke J, Petersen PE. Evidence for dental cariesdecline among children in an East European country (Hungary). Community Dent Oral Epidemiol 2000; 28: 155-160
- Boyce W, Den Besten P, Stamperdahl J, Zhan L,Jiang Y, Adler N, et al. Social inequalities in childhood dental caries: the convergent roles of stress, bacteria and disadvantage. Soc Sci Med 2010; 71:1644-1652.
- Edelstein BL. Disparities in Oral Health and Accessto Care: Findings of National Surveys. Ambulatory Paediatrics. 2002;2:141-147.
- Al-Shalan TA. Saudi parents knowledge of andattitude towards the prevention of dental caries. Saudi Dent J. 2003;15:2-10.
- Slavin R, Smith D. The Relationship betweenSample Sizes and Effect Sizes in Systematic Reviews in Education. Educational evaluation and policy analysis. 2009;31:500-506.
- Senior lecturer, Community dentistry Department. Baqai dental college. Baqai Medical University.Karachi.Pakistan
- Director of Post graduate Studies and Research, Associate Professor and HOD, Department of Periodontology. Ziauddin University. Karachi. Pakistan 3. Lecturer,Department of Periodontology Ziauddin University Karachi. Pakistan
Corresponding author: “Mohammad Ali Leghariâ€
Email: dralileghari@gmail.com Cell# 03212141488